 |
 |
|
|
| ||||||||
|
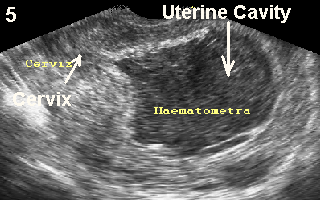
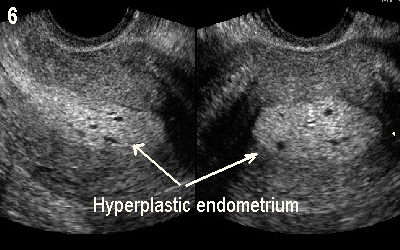
Other endocrine dysfunctionsFunctional integrity of the HPO axis may be adversely affected even by the most subtle changes in other pituitary or target endocrine glands hormones. The correlated problems we most see as gynaecologists are associated to: · Thyroid gland dysfunction;· Hyperprolactinaemia;· Adrenal gland dysfunction;· Polycystic ovary syndrome (PCOS).Thyroid dysfunctionThyroid gland disorders are very common in women, and may cause different types of menstrual irregularities. Accordingly, a high degree of suspicion should be exercised. This is especially so when dealing with women >40 years old, and younger ones with similar family history. The function of the HPO axis is closely interlinked to that of the thyroid gland. Both, an underactive or overactive thyroid gland may affect ovulation by different means. TSH and gonadotrophins are glycoproteins with very similar structure. They even have identical amino acids sequence in their alpha chains. In vitro studies showed that thyroid hormones increased granulosa cells division, and enhanced their production of oestradiol. This was more noticeable for T3 than T4 (23). On the other hand, any change in the level of circulating oestrogens can also affect the thyroid gland. High oestradiol blood levels stimulate the liver to produce more thyroxine binding globulin which is the carrier molecule of thyroxine. Normally this leads to a drop in the level of free T4, calling on the thyroid gland to produce more thyroxine to compensate for that effect. This can be seen during pregnancy, or after exogenous administration of oestrogens including the combined contraceptive pills, and hormone replacement therapy.Childhood hypothyroidism may lead to delayed or precocious puberty, as discussed in Chapter 2. In the later case, secondary stimulation of the pituitary gland by TRH increases gonadotrophins production. Elevation of TRH can also lead to hyperprolactinaemia, and affects the HPO axis adversely. There is also reduced production of SHBG in cases of hypothyroidism, which leads to increased levels of free testosterone and oestradiol in circulation. High free androgens are converted to oestrone in the hypothalamus which can modulate GnRH generation. Nonetheless, gonadotrophins levels may be normal, but a blunted or delayed response of LH to GnRH stimulation may be seen in patients with hypothyroidism (24; 25)On the other hand, high thyroxine levels increase the pituitary gonadotrophs sensitivity to GnRH with significant increase in the production and secretion of LH during both phases of the cycle. A similar effect has been reported for FSH, but not by all investigators. This effect may be sustained for up to 4 months after initiating antithyroid treatment, which explains the lag period between normalisation of thyroid indices and resumption of normal ovulatory function. High thyroxine blood levels also increase the production of SHBG by the liver which reduces the metabolic clearance of oestradiol. There is also increased production of oestradiol by the granulosa cells in response to thyroxine (22). Accordingly, there is 2-3 folds increase in oestradiol level during the follicular and luteal phases of the cycle. There is also increased production of testosterone and androstenedione, with significant increase in their conversion rates to oestradiol and oestrone respectively. Even with regular menstrual cycles, progesterone levels during the luteal phase were found to be low in women with hyperthyroidism compared to control groups.HyperprolactinaemiaCirculating human prolactin can be found in 3 different molecular weights of 23, 60 and 100 kilodaltons. They are called little, big and big-big prolactin respectively. The major circulating form is little prolactin which is also the biologically active hormone. The big-big variety is known as macroprolactin (26), and is made of little prolactin and immunoglobulin G antibody. This complex structure interferes with the hormone/receptor interaction (27) and renders prolactin biologically inactive. Macroprolactinaemia may be found in 18-42% of patients with high prolactin blood levels (28). These patients are usually asymptomatic and have regular menstrual cycles, as the hormone is biologically inactive. Recently, a suggestion has been made to test the biological activity of prolactin in all patients with hyperprolactinaemia, as this may affect the management plan (29). This practice is not yet universal and symptomatic patients with hyperprolactinaemia are treated accordingly. The rest of the text in this section relates to the biologically active prolactin.About 15% of amenorrhoeic women have increased prolactin blood levels, which can affect the HPO axis directly at all levels. Increased prolactin production can follow any of the following conditions:· Prolactin producing pituitary tumours may be micro or macroadenomas, with <10 mm and >10 mm size respectively. Such tumours are usually autonomous, and the amount of prolactin produced depends on their size. They should be excluded with MRI during investigations of hyperprolactinaemia.· Certain drugs functionally block the inhibitory effect of dopamine on the pituitary gland lactotrophs, allowing autonomous production and release of prolactin. Oestrogens have been shown to restrict access of dopamine into the lactotrophs granules. This explains the exaggerated prolactin response after TRH stimulation test following oestrogen medication.· Traumatic stalk transection or disruption of the vascular connections between the hypothalamus and pituitary gland by a craniopharyngioma, pituitary tumour, or any other intracranial growth can prevent delivery of prolactin inhibitory factor to the pituitary gland.· Increased production of prolactin by the pituitary gland may follow increased production of TRH due to hypothyroidism. It can also follow the use of such drugs as metoclopramide and cimetidine which act as dopamine antagonists, and allow more prolactin secretion by the pituitary gland. This effect can also be augmented by prior exposure to oestrogen medication. It is interesting that the effect of cimetidine on prolactin secretion is blunted in patients with hyperthyroidism (30). This may be an indication that cimetidine affects prolactin secretion by more than one means. Chronic oestrogen medication can also enhance prolactin secretion, in isolation, by increasing lactotrophs mitotic activity and number. Other conditions which can increase prolactin secretion include nipples manipulation, chest surgery, herpetic inflammation of the intercostal nerves and renal failure.· Hypothalamic dopamine deficiency may follow inflammatory brain condition such as sarcoidosis, arteriovenous malformations and medical treatment with drugs such as reserpine and alpha methyldopa.Hyperprolactinaemia can alter GnRH pulse generation, and ultimately reduce gonadotrophins production, mainly LH. Alteration or abolition of the LH surge may lead to inadequate ovulation, abnormal luteal phase, polymenorrhoea, polymenorrhagia and menorrhagia. Pituitary adenomas and craniopharyngioma are more likely to cause amenorrhoea, as they lead to very high prolactin levels with severe gonadotrophins deficiency and hypoestrogenic state. Moderate elevation in prolactin levels following hypothyroidism or drug medication can cause oligomenorrhoea and abnormal uterine bleeding in some patients, but may also cause amenorrhoea. It may also act directly at the ovaries and reduce the effect of gonadotrophins on the follicles at a post-receptor level. This can lead to inappropriate folliculogenesis, long follicular phase and abnormal ovulation. Low luteal phase serum progesterone may also follow an abnormal effect at post LH receptors level. The clinical effects of hyperprolactinaemia can be summarised as follows: Dopamine ® ¯ gonadotrophins production ® ¯ follicular stimulation ® ¯ steroidogensis ® ¯ oestradiol ® ¯ positive feedback mechanism ® ¯ LH surge ® anovulation/oligomenorrhoea ® amenorrhoeaHigh prolactin levels can also interfere with adrenal enzymatic activity leading to increased production of androgens, which have detrimental effects on the ovaries and endometrium. Changes in 3β-hydrtoxysteroid dehydrogenase activity may reduce the conversion of ∆5 precursors into ∆4 products. This leads to increased production of 17a-hydroxypregnenolone and DHEA-S, with the later precursor changed into more potent androgens in peripheral tissues. It is not usual for an isolated mild deficiency of this enzyme to cause total amenorrhoea. Patients are more likely to present with some hyperandrogenic symptoms and signs.Adrenal gland dysfunctionDetailed information about the adrenal hormones can be found in Chapter 4. In the context of amenorrhoea, women with adrenal dysfunction can fall into 2 major groups1. Enzymatic deficiencies which are autosomal recessive problems;2. Cushings syndrome which is a rare presentation in the gynaecology clinic.The lack of a strong evidence associating adrenarche to the onset of puberty in normal girls has been discussed in Chapter 2. Nonetheless, excessive production of adrenal androgens due to 21-hydroxylase deficiency may lead to precocious puberty. Severe untreated conditions can result in primary or secondary amenorrhoea due to the effects of very high androgens at different parts of the HPO axis, and the uterus. Women with 21-hydroxylase deficiency are more prone to develop secondary polycystic ovaries. They may also show signs of hyperandrogenisation including acne and excessive hair growth. The less common 11-hydroxylase deficiency may cause similar problems, with an occasional added risk of high blood pressure. Deficiency of 17a-hydroxylase occurs in 1: 50,000 to 1: 100,000 newborns (31). It usually occurs in combination with 17/20 lyase enzymatic deficiency, as they are controlled by the same cytochrome P450c17 enzyme. Nonetheless, they might occur separately depending on the type of mutation (32). It has more dramatic effects than the other two enzymatic deficiencies mentioned before. Deficiency of 17a-hydroxylase reduces or even totally blocks the conversion of progesterone to 17a-hydroxyprogesterone, and pregnenolone to 17a-hydroxypregnenolone. With reduced synthesis of 17a-hydroxyprogesterone, less 11-deoxycortisol and cortisol will be produced. Deficiency of 17/20 lyase enzymatic activity will compound matters further by reducing the conversion of the available 17a-hydroxyprogesterone and 17a-hydroxypregnenolone to androgens, which are the substrates for oestrogens. The ultimate clinical outcome of these changes will be:· Failure of cortisol production will lead to increased production of ACTH, with excessive stimulation of the adrenal gland and further accumulation of the pre-block precursors. Excessive progesterone will be converted more readily to deoxycorticosterone and corticosterone. This may lead to hypertension and hypokalaemic alkalosis. The age of onset and degree of severity of hypertension vary between the affected individuals (33)· Failure to produce androgens and oestrogens will result in failure to develop secondary sexual characteristics, and primary amenorrhoea.The biochemical picture will be high levels of FSH, LH, progesterone, deoxycorticosterone and corticosterone, but low oestradiol level. Aldosterone and plasma rennin activity may also be reduced. The ovaries may show multicystic pattern, but ovarian biopsies showed no evidence of follicular maturation. Despite failure of spontaneous follicular growth, patients with 17a-hydroxylase (34) and isolated 17/20 lyase (35) enzymatic deficiencies had positive response to exogenous gonadotrophins stimulation with adequate follicular growth, oocyte maturation and fertilisation during in vitro fertilisation programmes. These studies demonstrated the need for a proper diagnosis to differentiate these patients from others with high FSH and low oestradiol levels due to primary ovarian failure.Individuals with 46XY karyotyping and severe or homozygous 17b-hydroxysteroid dehydrogenase 3 mutations may be born with external female genitals, and are raised as females. They will fail to menstruate, and develop hyperandrogenic habitat at the time of puberty. This topic will be discussed in more details in Chapter 4.Cushings syndrome is usually diagnosed in a medical department rather than a gynaecology clinic. The main endocrine problems are excessive ACTH induced, or independent cortisol production by the adrenal glands. There is also loss of the cortisol circadian rhythm, together with the hypothalamo-pituitary-adrenal negative feedback mechanism. The clinical manifestations may be subtle in the early stages and many of the symptoms are shared by other endocrine dysfunctional conditions. The full blown picture may show central obesity, purple wide striae, hyperandrogenisation, facial plethora, mooning of the face, muscle wasting, diabetes and high blood pressure. Patients may also present with secondary amenorrhoea, even at the early stages of the syndrome. Accordingly, it should be kept in mind during the investigations of patients who present with amenorrhoea associated with any of the other symptoms or signs described before. It is important not to confuse this condition with the pseudo Cushing state related to excessive alcohol abuse and depression. These patients present with clinical and biochemical changes reminiscent of Cushing syndrome. They may even fail to respond to a dexamethasone suppression test. Treatment is different in these cases, and should only target the two underlying problems.Polycystic ovary syndromeThis is the most common female endocrine disorder and has been reported in 3.5-11.2% of all women. Almost 50% of all female endocrine problems are related to PCOS. The spectrum of symptoms includes hyperandrogenisation., anovulation, obesity, and infertility. Menstrual dysfunction is variable, with oligomenorrhoea being most common, but primary and secondary amenorrhoea may be seen. A new consensus has been agreed for the diagnosis of PCOS in 2003 (36), but still needs to gain universal approval. The Rotterdam expert group stated that PCOS is an ovarian dysfunctional condition characterised by hyperandrogenism, anovulation and the presence of 12 cystic areas in one or both ovaries. Other causes of hyperandrogenic states should be excluded first, before making the diagnosis. A more detailed account will be given about PCOS in Chapter 6.Management of amenorrhoeaThorough medical history should be taken and physical examination and investigations should be performed according to the patients age, pubertal development, general phenotype and the presence or absence of other endocrine physical signs. The main objectives should be to exclude medical problems which can affect the patients general health. This is especially so for intracranial, ovarian or adrenal tumours. The management plan ought to have purposeful treatment oriented objectives. It must seek to distinguish between the following conditions:1. Hypogonadotropic hypogonadism;2. Hypergonadotropic amenorrhoea with or without gonadal dysgenesis;3. Hyperandrogenic amenorrhoea;4. Anatomical amenorrhoea.The following action plan is suitable for most patients, and can be modified as necessary to suit each individual case:· Personal biodata including weight, height, arms span and blood pressure should be recorded.· Tanners breast and pubic hair staging should be performed.· Look for hyperandrogenic signs, central obesity, and purple wide striae.· Signs of hypo or hyperactive thyroid gland should be ascertained.· The vulva should be inspected in cases of primary amenorrhoea.· Digital vulvar examination of sexually active patients with primary amenorrhoea should be done.· Neurological examination including the optic discs and visual fields should be conducted.· Transabdominal and transvaginal ultrasound pelvic scan examinations may show the presence or absence of the uterus and ovaries. Distension of the uterus and vagina with blood may be demonstrated in cases of haematometra and haematocolpos, secondary to genital tract obstruction. These are the findings mostly seen in younger patients. Few women with amenorrhoea or dysfunctional uterine bleeding may show polycystic ovaries and the endometrium may be hyperplastic and thick. This is a pattern seen more often in obese women as shown in figure 6.
Intrauterine adhesions can show in many different ways including a thin endometrium with bright neighbouring echoes, as shown in figure 6. Loss of the endometrial / myometrial interphase may be the only ultrasonic finding. This could be more discernable during the luteal phase of the cycle because of the contrast between the remaining part of the echogenic secretory endometrium and the normally hypoechoic inner part of the myometrium. The diagnosis is best concluded with saline infusion sonohysterography. Failure of uterine distension may indicate total obliteration of the cavity. Alternatively, distortions of the cavity with echogenic bridges, or failure of a specific part of the cavity to distend with saline may be seen. Saline infusion sonohysterography is an outpatient procedure which can be used in isolation in most cases, or in conjunction with office hysteroscopy. It should be performed under aseptic conditions, and should be covered with antibiotics.
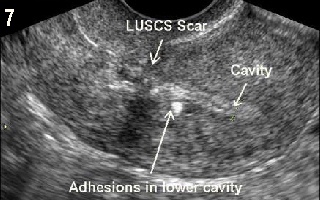
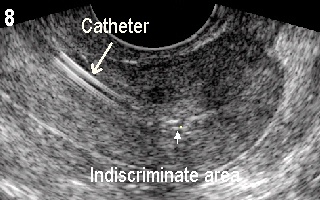
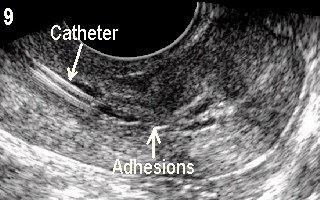
Figure 8 shows an indiscriminate endometrial / myometrial interface, marked by an arrow head, which proved to be due to intrauterine adhesions as shown by saline infusion sonohysterography in Figure 9. The intact part of the cavity is revealed by the hypoechoic saline with adhesions shown as bright bridges dividing the cavity. The catheter used for saline infusion is shown as two bright parallel lines in the cervical canal.
· MRI of the pituitary gland and brain are necessary in cases of hyperprolactinaemia, and in cases of delayed and precocious isosexual puberty. This is especially important in patients with neurological symptoms, or abnormal findings on neurological examination. Plain skull X-ray examinations are not sensitive enough to be used for this purpose.· Peripheral karyotyping is important in cases of primary or secondary amenorrhoea with high FSH blood levels. It is also useful in cases of suspected androgen receptor insensitivity (46XY) and Mayer-Rokitansky-Küster-Haϋsers syndrome (46XX).· X-ray of the left hand and wrist for bone age should be requested for women with delayed or precocious puberty, and the film compared to a standard atlas.· An endocrine profile should be requested including:o FSH, LH, and oestradiol can differentiate between hypo and hypergonadotropic amenorrhoea;o TSH and free T4 are needed to investigate thyroid function.o Testosterone, androstenedione and SHBG are useful in cases of hyperandrogenic amenorrhoea and in cases suspected of androgen insensitivity syndrome. Very high testosterone levels may point towards ovarian or adrenal tumours.o 17-hydroxyprogesterone is the main precursor necessary for the diagnosis of 21-hydroxylase deficiency.o DHEA-S, androstenedione and cortisol should be assessed, as necessary, to give more information about the adrenal gland. Very high DHEA-S may indicate the presence of an adrenal tumour.· Pituitary dynamic tests for FSH, LH, TSH, ACTH and growth hormone can be performed to test the integrity of all trophic hormones in cases suspected of hypopituitarism.· Stimulation of the adrenal gland with a bolus dose of synacthen should be utilised to diagnose 21-hydroxylase enzymatic deficiency in marginal or doubtful cases. Excessive increase in the level of 17-hydroxyprogesterone will confirm the diagnosis. A similar test is also available for the less common 11β-hydroxylase deficiency with metyrapone.Treatment of primary and secondary amenorrhoeaThe main objective of managing patients with amenorrhoea is to exclude serious organic causes which may affect their future wellbeing. Identifying patients with hypo or hypergonadotrophic amenorrhoea is the next important objective. It is also important to remember that endocrine glands are biochemically interlinked, and a derangement in one gland may affect many others. Accordingly, the diagnostic workup should be thorough and purposeful to detect such changes. A good example is the elevation of prolactin level in response to hypothyroidism. Treating hyperprolactinaemia in such cases entails dealing with the causative hypothyroidism first. Management of amenorrhoeic patients in general depends on the patients age, definitive diagnosis, associated symptoms and fertility demands as shown in the following examples:· Development of young hypogonadal pubertal girls should be enhanced with small doses of oestrogen to allow linear growth and development of secondary sexual characteristics. The dose should be maintained and a progestogen should be added to allow regular endometrial shedding, once the patient is fully developed. This will also allow the normal attainment of maximum bone density by the age of 20 years, and prevent osteoporosis. Dysgenetic gonads should be removed in individuals with a Y chromosome, to guard against malignant transformation. Induction of ovulation with gonadotrophins is the standard treatment in patients with hypogonadotropic hypogonadism, when pregnancy is desired. Pulsatile GnRH medication is also possible in cases of hypothalamic amenorrhoea with an intact pituitary gland.· Patients with hyperprolactinaemia usually respond well to bromocripine which is a dopamine D1 and D1 receptor agonist. It should be started in a small dose of 2.5 mg every day with food. The dose should be increased slowly over few days and titrated against prolactin level. A positive response of 80% is expected in cases of amenorrhoea caused by hyperprolactinaemia. Some menstrual activity may resume after a short period of time, but it usually takes many weeks or months before a full ovulatory response is seen. Accordingly, additional medication to stimulate ovulation should not be rushed. Bromocripine is indicated even in cases of pituitary macroadenoma as a first line of management. The tumour size may shrink, which makes it easier to remove surgically. Tumours which already involved neighbouring structures, especially the optic chiasm need surgical decompression first. Regular follow up with MRI and visual field examinations should also be done together with serial estimations of prolactin blood levels. There is a risk of pituitary tumours increasing in size during pregnancy. Longer acting dopamine agonists are available if bromocripine is not well tolerated, and for maintenance purpose for long periods of time in patients who are not keen to get pregnant. Single weekly doses of cabergoline (dostinex 0.5 - 1.0 mg) can improve compliance with taking the drug.· Patients with hypo and hyperthyroidism should be managed accordingly. Thyroxin treatment should be started with a small dose and built up against TSH levels, to reduce side effects especially cardiac ones. It is important to remember that menstrual function and more importantly regular ovulation may take much longer time to resume after correction of the peripheral blood levels of thyroid indices. Similarly, other medications to induce ovulation should not be rushed. The relationship between hypothyroidism and hyperprolactinaemia has been mentioned before.· Eating disorders are common in young women, and should be treated as psychological rather than endocrine problems. These patients usually have negative body image, and intense fear of gaining weight. They may also suffer from depression, anxiety and obsessive compulsive disorders. Treatment should focus on cognitive behavioural therapy and behaviour modification, personal and family counselling, nutritional advice, as well as individual and group counselling sessions. Antidepressants and hormone replacement therapy should be prescribed in severe cases suffering from depression, and to prevent bone loss respectively.· A diagnosis of hypothalamic dysfunction is usually made in amenorrhoeic patients with normal gonadotrophins, oestrogens, prolactin, thyroid indices and adrenal hormones. This is fitting with the WHO group 2 classification of amenorrhoea. Patient with PCOS can show clinical and / or biochemical hyperandrogenisation. Treatment is almost the same in both groups depending on the following parameters as far as menstruation is concerned:1. Patients who are not keen to get pregnant should have regular progestogens withdrawal bleeding every 6-8 weeks, to prevent endometrial hyperplasia. Alternatively, they can be offered an oral contraceptive pill to have monthly withdrawal bleeding, and prevent unwanted pregnancies at the same time.2. Patients who wish to conceive should be offered induction of ovulation with clomiphene citrate as a first choice. Gonadotrophins injections can be used when a good response is not attainable. They are more expensive, and need expert serial monitoring to reduce the risk of excessive response and hyperstimulation.SummaryIt is evident that primary and secondary amenorrhoea share many similar causes, and fit into almost identical management strategies. A logical clinical, hormonal and imaging approach will elucidate most cases with minimal need for advanced investigations. The sensitivity of the problem especially with primary amenorrhoea in young pubertal girls and in older patients who wish to get pregnant makes it necessary for all gynaecologists to have a clear management plan, as stated before. Dealing with the anatomical abnormalities involved with primary amenorrhoea can pose greater difficulty, and liaison with a gynaecologist experienced in this form of surgery is important. As a whole, a multidisciplinary approach will be needed to cover the different needs of these patients.References1. Herman Giddens ME, Slora EJ, Wasserman RC, Bourdony CJ et al. Secondary sexual characteristics and menses in young girls seen in office practice: a study from the Paediatric Research in Office Settings network. Pediatrics. 1997; 99(4): 505 - 512. 2. Kiningham RB, Apgar BS, Schwenk TL. Evaluation of amenorrhea. Am Fam Physicians. 1996; 53(4): 1185 - 1194. 3. Timmreck LS, Reindollar. Contemporary issues in primary amenorrhoea. Obstet Gynecol Clin North AM. 2003; 30(2): 287 - 302. 4. Pettersson F, Fries H and Nillius SJ. Epidemiology of secondary amenorrhoea; incidence and prevalence rate. Am J Obstet Gynecol 1973; 117(1): 80 - 86 5. Brundu B, Loucks TL, Adler LJ, Cameron JL and Berga SL. Increased cortisol in the cerebrospinal fluid in women with functional hypothalamic amenorrhoea. J Clin Endocrinol Metab 2006; 91(4); 1561 - 1565. 6. Gadpaille WJ, Sanborn CF and Wagner Jr WW. Athletic amenorrhoea, major affective disorders, and eating disorders. Am J Psychiatry 1987; 144: 939-42 7. Wildt L, Leyendecker G, Sir-Petermann T and Waibel-Treber S. Treatment with naltrexone in hypothalamic ovarian failure: induction of ovulation and pregnancy. Hum Reprod 1993; 8(3): 350- 358. 8. Product Monograph. Depoprovera. Pfizer, Canada Inc 2006 9. Jaffe RB, Plosker S, Marshall L and Martin MC. Neuromodulatory regulation of gonadotropin-releasing hormone pulsatile discharge in women. Am J Obstet Gynecol 1990; 163(5 Pt 2): 1727 - 1731. 10.Xiao E, Xia-Zhang L, Thornell D, Ferin M. Interleukin-1 stimulated luteinising hormone release during the midfolliculr phase in the rhesus monkey: a novel way in which stress may influence the menstrual cycle. J Clin Endocrinol Metab 1996; 81: 2136 2141. 11.Quigley ME, Sheenah KL, Casper RF, Yen SSC. Evidence for increased dopaminergic and opioid activity in patients with hypothalamic hypogonadotropic amenorrhea. J Clin Endocrinol Metab 1980; 50(5): 949 - 954. 12.Sachar EJ, Hellman L, Roffwarg H, Halpern FS, Fukushima. DK, Gallagher TF. Disrupted 24 hour patterns of cortisol secretion in psychotic depression. Arch Gen Psychiatry 1973; 28: 19 - 24. 13.Amsterdam JD, Winokur A, Abelman E, Lucki I and Rickels K. Cosyntropin (ACTH alpha 1-24) stimulation test in depressed patients and healthy subjects. Am J Psychiatry 1983; 140: 907 - 909. 14.Ferin M. The hypothalamic-hypophyseal-ovarian axis and the menstrual cycle. Glob libr womens med.; (ISSN: 1756-2228) 2008; DOI 10.3843/GLOWM.10283. 15. Kwok C, Tyler-Smith C, Mendonca BB, Hughes I, Berkovitz GD, Goodfellow PN, Hawkins JR. Mutation analysis of the 2 kb 50 to SYR in XY female with XY intersex subjects. J Med Genet 1996; 33: 465 468. 16.Papagianni V, Deligeoroglou E, Makrakis E. Response to hormonal treatment of young females with primary or very premature ovarian failure. Gyn Endocrin 2011; Early on Line; 1 9. 17. Abdel Gadir, A. and Ramadan, AA. Abnormal ovarian cell line: A cause for ovarian failure. British Journal of Obstetrics and Gynaecology 1990, 97, 446 - 448. 18.Marozzi A, Vegetti W, Manfredini E, Tibiletti MG, Testa G, Crosignani PG, Ginelli E, Meneveri R and Dalpra L. Association between idiopathic premature ovarian failure and fragile X permutation. Hum Reprod 2000; 15: 197 - 202. 19.Sherman SL. Premature ovarian failure in fragile X syndrome. Am J Med Genet 2000; 97: 189 - 194. 20.Bines J, Oleske DM and Cobleigh MA. Ovarian function in premenopausal women treated with adjuvant chemotherapy for breast cancer. J Clin Oncol 1996; 14: 1718 - 1729. 21.Minton SE and Munster MD. Chemotherapy-induced amenorrhoea and fertility in women undergoing adjuvant treatment for breast cancer. Cancer Control 2002; 9(6): 466 - 472. 22.Abdel-Gadir A, Francis N, Oyawoye O and Chander B. Secondary amenorrhoea with high inhibin B level caused by parasitic ovarian leiomyoma. Gynecol Endocrinol. 201; 26(2): 93 95. 23.Misiti S, Falzacappa CV, Mangialardo C, Bucci B, Raffa S, Silvestrini G, Stigliano A and Toscano V. Effects of thyroid hormones on ovary granulosa cells: regulation of proliferation, survival and function. Endocrine Abstracts (2009) 20 P623. European Congress of Endocrinology, Istanbul, Turkey, 25 April 2009, European Society of Endocrinology. 24.Distiller LA, Sagel J, Morley JE. Assessment of pituitary gonadotropin reserve using luteinising hormone-releasing hormone (LRH) in states of altered thyroid function. J Clin Endocrinol Metab 1975; 40: 512 - 515. 25.Valenti G, Ceda GP, Denti L. Gonadotropin secretion in hyperthyroidism and hypothyroidism. La Ric Clin Lab 1984; 14: 53 - 63. 26.Fahie-Wilson. The Macroprolactinaemia problem and its solution. South Med J 2006; 99: 1206. 27.Hattori N, Nakayama Y, Kitagawa K, Ishihara T, Saiki Y, and Inagaki C. Anti-prolactin (PRL) autoantibodies suppress PRL bioactivity in patients with macroprolactinaemia. Clin Endocrinol (Oxf) 2008; 68: 72 76. 28.Kavanagh-Wright L, Smith TP, Gibney J, and McKenna TJ. Characterization of macroprolactin and assessment of markers of autoimmunity in macroprolactinaemic patients. Clin Endocrinol (Oxf) 2009; 70: 599 605. 29.Kostrzak A, Warenik-Szymankiweicz A and Meczekalzki B. The role of serum prolactin bioactivity evaluation in hyperprolactinaemic women with different menstrual disorders. Gyn Endocrinol 2009; 25(12): 799 806. 30.Kamijo K, Saito A, Kato T, Kawasaki K, Suzuki M, Yabana T, Yachi A, Wada T. Effect of cimetidine on prolactin secretion in normal controls and hyperthyroid patients. Endocrinol Jpn 1982 ; 29(2): 177 - 181 31.Costa-Santos M, Kater CE, Auchus RJ. Two prevalent CYP17 mutations and genotype-phenotype correlations in 24 Brazilian patients with 17-hydroxylase deficiency. J Clin Endocrinol Metab 2004; 89: 49 - 60. 32.Ergun-Longmire b, Auchus R, Papari-Zareei M, Tansil S, Wilson RC and New MI. Two novel mutations found in a patient with 17a-hydroxylase enzyme deficiency. J Clin Endocrinol Metab 2006; 91(10): 4179 - 4182. 33.Rosa S, Duff C, Meyer M, Lang-Muritano M, Balercia G, Boscaro, Kemal Topaloglu, Mioni R, Fallo F, Zuliani L, Mantero F, Schoenle EJ and Biason-Lauber A. P450c17 Deficiency: Clinical and Molecular Characterization of Six Patients. J Clin Endocrinol Metab 2007; 92(3): 1000 1007. 34. Rabinovici J, Blankstein J, Goldman B, Rudak E, Dor Y, Pariente C, Geier A, Lunenfeld B and Mashiach S. In vitro fertilisation and primary embryonic cleavage are possible in 17a-hydroxylase deficiency despite extremely low intrafollicular 17a-oestradiol. J Clin Endocrinol Metab 1989; 68: 693 - 697. 35.Pellicer A, Miró F, Sampaio M, Gomez E and Bonilla-Musoles A. In vitro fertilization as a diagnostic and therapeutic tool in a patient with partial 17, 20 desmolase deficiencies. Fertil Steril 1991; 55: 970 - 975. 36.Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril 2004; 81(1): 19 25. |
|||||||||||||||||||||||||||||||||||
| Site Map |